

Dynamics of ACS: Top 12 ECGs of 2022 (Part 2)
Dynamics of ACS: Top 12 ECGs of 2022 (Part 2)
ECG Experts Uncover their Most Fascinating ECG Cases of the Year

This is Part 2 of this exciting ECG series. This week we have 3 MEGA cases of three true ECG experts breaking down the dynamic electrocardiographic changes in ACS!
Use the following quick links to navigate to the expert ECG cases quickly:
Sam Ghali’s ECG: 55F with a chief complaint of heartburn.
Pendell Meyer’s ECG: Two middle-aged patients with acute chest pain. Is it OMI?
Emre Aslanger’s ECG: 40M with excruciating chest pain.
Go through Part 1 ECG cases first.
1. Sam Ghali (@EM_RESUS)
Background
A 55-year-old woman with the chief complaint: “Heartburn”. Symptoms started while drinking wine and eating chili. Took antacids with no relief.
The following two ECGs (20 minutes apart) were recorded:
ECG #1 in the pre-clinical setting
ECG #2 during the patient’s admission to the hospital
Suggest your interpretation in the comments below, before looking at the expert breakdown!

Expert breakdown
I believe putting Sam’s expert interpretation of this ECG into written words severely undermines the educational value and excitement of this case. Please listen to him breaking it down in this video instead:

Meet Sam
Sam Ghali, MD is a board-certified emergency medicine physician and Assistant Professor of Emergency Medicine at Louisiana State University. He is an excellent and active ECG and EM educator with a massive community on Twitter.
RH’s addition: “I’ve never heard someone describe T-waves with 6 or more completely fitting adjectives. Is Sam also a voice artist in his spare time? I don’t know… His videos and his excitement for this field are truly inspiring.”
2. Pendell Meyers (@PendellM)
Background
Here is a quick comparison/quiz post. It will be easy for long-time Dr. Smith’s blog readers. The two ECGs below are both from middle-aged patients with acute chest pain.
Do either, neither, or both patients have an ECG diagnostic of OMI, warranting emergent reperfusion therapy? Comment below before looking at the interpretations.

Expert breakdown
Patient #1 has a totally normal, normal variant ECG. There is no OMI. There is about 1mm of STE in all inferior leads (importantly without any reciprocal STD or TWI in aVL), and additional STE in V4-V6. There are J waves. None of the T waves are hyperacute. It is NOT inferolateral OMI. It is certainly NOT evidence of pericarditis. It is normal. The patient was ruled out for AMI with serial troponins.
Patient #2 has unequivocal (i.e., definite!) acute inferior-posterior OMI. There is maybe 1mm of STE in the lead III, and only a touch of STE in II and aVF, but with diagnostic reciprocal STD in aVL (unexplained by the normal QRS complex). The inferior T waves are subtly hyperacute because the diagnostic context tells me that their area is increased from what the baseline must be. The diagnosis is made even easier by the concomitant posterior OMI, evidenced by STD maximal in V2-V3 and unexplained by the normal QRS complex. The ECG is diagnostic of inferior-posterior acute transmural injury, almost certainly due to acute thrombotic coronary occlusion or near occlusion (once in a while, another etiology such as occlusive spasm, etc. will achieve the same physiologic occlusion).
Patient #2 sadly had a delay in the identification of her acute RCA occlusion because her ECG "didn't meet STEMI criteria". No posterior leads were ever done (as is common in these missed cases). The RCA was eventually stented. She survived the hospitalization and likely has increased long-term mortality and morbidity compared to her outcome with immediate reperfusion.
Further learning points and additional expert interpretation of Ken Grauer (from Part 1 of this series) is available on Dr. Smith’s ECG blog.
Meet Pendell
(Harvey) Pendell Meyers, MD is an assistant professor of Emergency Medicine at Carolinas Medical Center, North Carolina, and co-editor of Dr. Smith’s ECG blog. He is the co-author of the OMI manifesto, driving the paradigm shift from STEMI/NSTEMI to OMI/NOMI paradigm.
RH’s Addition: “Pendell is one of the few (humans) on this planet who can spot OMI with unmatched precision in a matter of 5 seconds. Please trust me I have seen this in action, timed and tested him extensively.”
3. Emre Aslanger (@AslangerE)
Background
A 40-year-old man presents with excruciating back pain which started 1 hour ago. His medical history is unremarkable except a similar pain occurred 4-5 times in the previous 3 months with less intensity, short duration, and unrelated to exertion. He visited an outpatient clinic for it, and an echocardiogram and exercise stress test was normal. He has 40 packs-year of smoking history. There was no premature cardiovascular diseases or sudden death in his family. He denies taking any medication.
On his physical examination, cardiac and pulmonary auscultation was completely normal. Peripheral pulses were all palpable. Blood pressure: 130/80 mmHg, heart rate: 45/min, respiratory rate: 18/min, SaO2: %98, body temperature: normal.
As he seemed very agitated, fentanyl and diazepam were given.
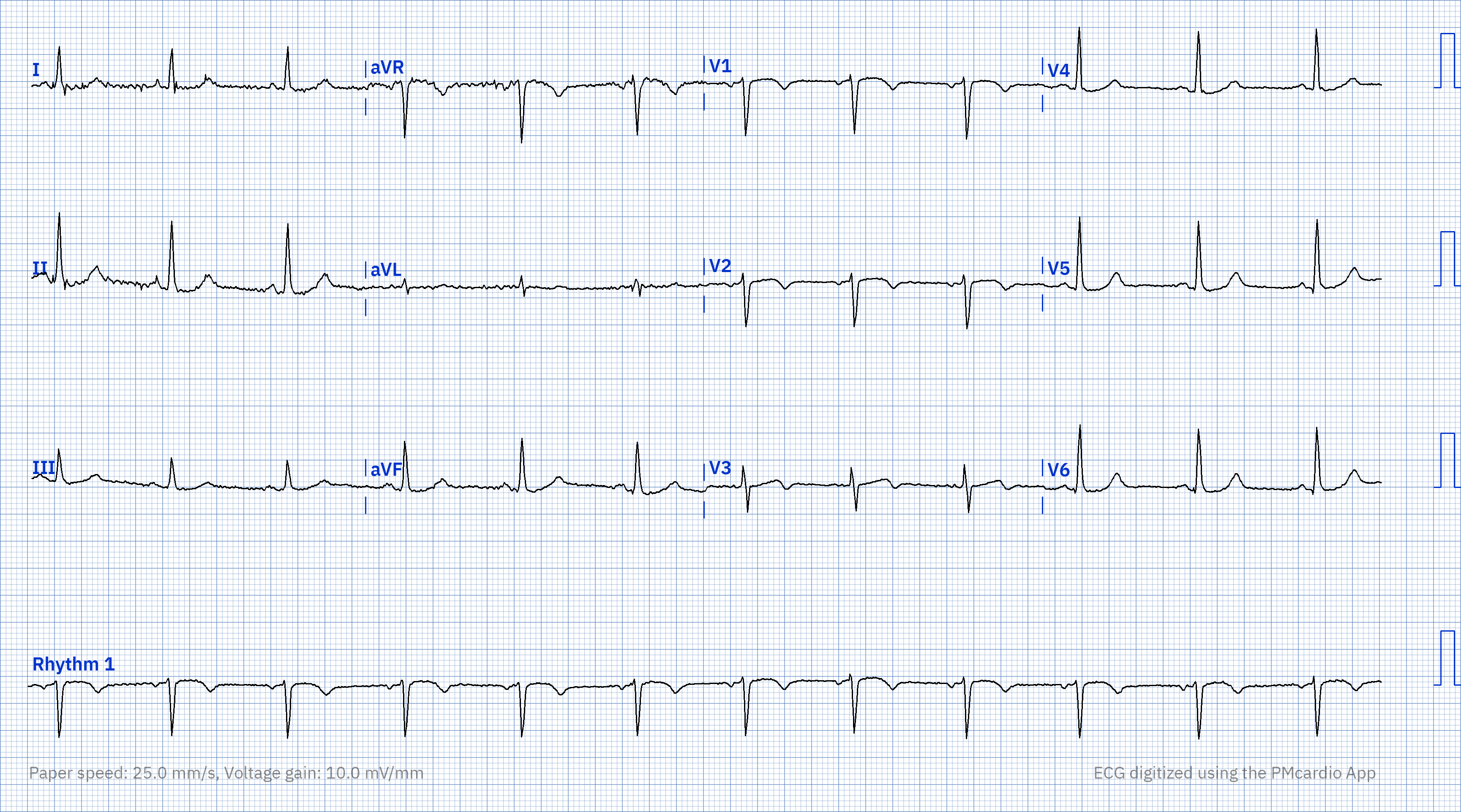
His first electrocardiogram (ECG) is given below:

Expert breakdown
Sinus bradycardia.
There are some ST-segment elevations (STE) in V2-5 and lead II, III, aVF.
No reciprocal ST-segment depression (STD).
QT is short, R wave amplitudes are preserved.
For subtle anterior OMI, Smith's 4-variable and Aslanger's simplified formulas both supports benign variant STE.
For subtle inferior OMI, there is no STD in aVL or lead I.
In summary, some subtle findings which do not fit into a pattern therefore may be nonspecific ECG changes that are encountered every day.
His pain is now settled a bit, around 4/10 and first troponin turned out to be 12 ng/L (normal <14 ng/L). Second troponin at 1h comes 20 ng/L. It is above the normal limit and there is a significant change.
With ongoing pain, without any clinical evidence of OMI, the cardiologist thinks NSTEMI and admits the patient to the step 1 coronary care unit. His ECG on arrival to the CCU:

This ECG was taken with a different machine but there seems to be one dynamic change: There is T wave inversion in lead III and Q wave is still there. This is a very subtle change but cannot be anything other than an acute coronary event. The pain is still ongoing. Therefore cath lab is activated.
Continue reading this excellent learning case depicting the OMI paradigm in action on Dr. Smith’s ECG Blog.
Meet Emre
Emre Aslanger, MD is an associate professor and interventional cardiologist at Marmara University, Department of Cardiology, Istanbul, Turkey. He has coined the term Aslanger’s pattern, for acute inferior OMI in patients with concomitant multi-vessel disease and is amongst the Top 3 drivers of the OMI/NOMI paradigm.
How many ECGs were you able to interpret correctly before looking at the expert breakdown?
If you liked this Part, please check out Part 1 of the series where expert unveil their favorite ECGs of 2022.
Robert Herman, MD is a physician and scientist with a background in technology and expertise in AI and machine learning. He is the Co-founder of Powerful Medical, where he serves as the Chief Medical Officer and leads the research and clinical evaluation of AI-powered medical devices for diagnosing and managing cardiovascular diseases.
If you liked this, please click the🤍 below so other people will see this here on Substack and consider sharing the article.